
DIGITAL FATIGUE IN THE AGE OF SCREENS: EYE AND POSTURAL STRAIN AMONG 18–35-YEAR-OLD SCREEN USERS
Swizel Bagaji 1![]() , Roopa Rao 2
, Roopa Rao 2![]()
![]()
1 Student,
Author, Department of Community Resource Management, College of Home Science
Nirmala Niketan, (Affiliated to University of Mumbai), Mumbai – 20,
Maharashtra, India
2 Associate
Professor, Mentor Department of Community Resource
Management, College of Home Science Nirmala Niketan, (Affiliated to University
of Mumbai), Mumbai – 20, Maharashtra, India
|
|
|
ABSTRACT |
|
|
The pervasive
use of digital devices has led to a sharp rise in screen-related health
concerns, particularly among young adults. This study investigates the
growing phenomenon of Computer Vision Syndrome (CVS) and associated postural
strain among individuals aged 18–35 years, who are heavily reliant on screens
for work, communication, and entertainment. With symptoms ranging from dry
eyes, blurred vision, and headaches to neck and shoulder pain, digital
fatigue poses a multifaceted risk to long-term well-being and productivity.
An explorator research targeting 160 participants
was conducted employing a structured questionnaire, postural assessments via
the Ovako Working Posture Analysis System (OWAS).
Results revealed that 78.7% experienced symptoms of eye strain, including
dryness, burning sensation, and blurred vision. 68.1% reported headaches or
discomfort during or after screen usage. Musculoskeletal issues such as neck
stiffness (59.4%) and shoulder discomfort (55%) were also prevalent. OWAS
analysis confirmed that the majority of users
exhibited moderate to high-risk postures, particularly while using mobile
devices or laptops without ergonomic adjustments. Awareness of digital
hygiene practices, such as the 20-20-20 rule or screen time breaks, was low
among respondents. The findings highlight the growing health burden posed by
digital fatigue among young screen users, exacerbated by lifestyle habits,
poor ergonomics, and limited awareness. The study calls for urgent
interventions in the form of structured awareness programs, digital wellness
education, and workplace or academic ergonomics audits. Promoting preventive behaviour, proper posture, and regular eye care can
significantly reduce the risk of long-term visual and musculoskeletal
complications. |
|||
|
Received 12 April 2025 Accepted 02 May 2025 Published 14 June 2025 Corresponding Author Roopa Rao,
rooparao@nnchsc.edu.in DOI 10.29121/granthaalayah.v13.i5.2025.6191 Funding: This research
received no specific grant from any funding agency in the public, commercial,
or not-for-profit sectors. Copyright: © 2025 The
Author(s). This work is licensed under a Creative Commons
Attribution 4.0 International License. With the
license CC-BY, authors retain the copyright, allowing anyone to download,
reuse, re-print, modify, distribute, and/or copy their contribution. The work
must be properly attributed to its author.
|
|||
|
Keywords: Computer Vision Syndrome, Digital Eye
Strain, Postural Ergonomics, Screen Time Fatigue, Young Adults' Health |
|||
1. INTRODUCTION
As we enter the 21st century, the widespread use of computers and digital devices in homes and offices has increased health risks, particularly for the eyes. One prevalent condition, known as Computer Vision Syndrome (CVS) or digital eye strain, refers to a group of eye- and vision-related problems caused by prolonged exposure to screens, including computers, tablets, e-readers, and cell phones.
With the growing reliance on technology for work, education, and entertainment, CVS cases are rapidly increasing worldwide. The shift to remote work, online learning, and digital communication has significantly amplified screen time, making CVS a widespread modern-day health concern. According to recent studies, 50% to 90% of regular computer users experience CVS symptoms. Even children and adolescents, who spend hours on digital devices for gaming, social media, and online classes, are increasingly affected by the condition Kaur (2022).
Many individuals experience eye strain, dryness, irritation, blurred vision, and headaches after extended screen use. The discomfort often worsens with increased digital exposure, significantly affecting workplace productivity, academic performance, and leisure activities. Prolonged screen time strains the eyes and contributes to mental fatigue, reduced concentration, and overall discomfort Portello (2012).
Several factors contribute to CVS, including poor lighting, screen glare, improper viewing distances, and inadequate workstation ergonomics. The condition is further aggravated by decreased blinking rates when staring at screens, leading to dry and irritated eyes. Individuals with uncorrected vision problems, such as nearsightedness, farsightedness, or astigmatism, are at a higher risk of experiencing more severe symptoms. Moreover, the blue light emitted by screens may further intensify visual fatigue and disrupt sleep patterns Silvani (2022).
While eye health professionals have yet to find CVS as a cause of permanent eye damage, the associated pain and discomfort can significantly reduce overall well-being. With increasing digital dependence in daily life, CVS is becoming a major public health challenge, affecting people of all ages. If left unaddressed, it may lead to chronic eye problems and decreased quality of life in the long run.
Workplace stress among computer users has been confirmed in several surveys and studies, yet the role of ergonomic risk factors in contributing to this stress is rarely highlighted. With the increasing reliance on computers for work, education, and communication, individuals are spending prolonged hours in front of screens, making them highly susceptible to Computer Vision Syndrome (CVS) (American Optometric Association, 2024).
CVS characterized by eye strain, dryness, irritation, blurred vision, and headaches, is becoming a widespread issue among computer users (Computer Vision Syndrome - What is Computer Vision Syndrome?, 2025). The extended screen exposure, combined with poor workstation ergonomics—such as improper monitor height, inadequate lighting, and incorrect sitting posture—further exacerbates physical and mental fatigue Rao (2020). This not only impacts productivity and performance but also contributes to chronic stress, reduced concentration, and overall discomfort.
While organizations and institutions focus on efficiency, service quality, and customer satisfaction, the health and well-being of computer users must also be prioritized. Addressing ergonomic challenges by optimizing screen positioning, reducing glare, and promoting regular eye breaks can help mitigate CVS symptoms. This, in turn, can enhance productivity, reduce stress, and improve the overall quality of life for computer users.
2. Literature Review
The exponential rise in digital screen usage—driven by smartphones, laptops, tablets, and e-readers—has led to a global upsurge in cases of Computer Vision Syndrome (CVS), also known as Digital Eye Strain. CVS is defined (American Optometric Association, 2024) as “a group of eye and vision-related problems resulting from prolonged computer, tablet, e-reader, and cell phone use,” with common symptoms including eye fatigue, dryness, blurred vision, headaches, and musculoskeletal discomfort, particularly in the neck, shoulders, and back Falguni (2023).
Globally, the prevalence of CVS has become a public health concern. It is estimated that over 60 million people worldwide suffer from CVS Sheppard (2018), with symptoms found in over 70% of screen users, particularly those exposed for more than four hours daily. Rosenfield emphasized that smaller digital screens increase accommodative stress, contributing to visual fatigue and dry eye symptoms due to prolonged near work and decreased blink rates Rosenfield (2016). The concern has been amplified by post-pandemic shifts to online work, education, and entertainment, significantly increasing digital exposure among young adults.
In India, CVS is also highly prevalent. It is reported that 76% of IT professionals in Bangalore reported symptoms of CVS Agarwal (2021), with dry eyes and headaches as the leading complaints. A higher prevalence of 81.9% among medical and engineering students in Chennai, a group especially vulnerable due to long academic screen hours Lograj (2014). In a study on 320 computer users aged 20–50 years in Karnataka, a prevalence of 70.3%, with eyestrain (61.8%) and headaches (55.1%) being most common. Notably, only 12.4% of participants were aware of CVS, though a majority attempted self-regulated breaks Darshan (2019).
The musculoskeletal impact of screen overuse has also been well documented. A strong association between extended screen time (over five hours daily) and neck and upper back pain, largely due to poor posture and lack of ergonomic awareness Tanaya Naik (2022) Shrestha (2020). It was further added Anshel (2005) added that improper workstation design, inappropriate seating, and suboptimal screen angles often result in chronic discomfort, spinal misalignment, and fatigue-related syndromes.
Contributing factors to CVS are multifactorial. A systematic review and meta-analysis of 45 studies categorized causes into personal factors (e.g., poor posture, eye-screen distance, screen time duration), environmental factors (e.g., lighting, screen glare, brightness), and computer-related elements (e.g., slow refresh rates, contrast imbalance) Anbesu (2023). The study found a pooled CVS prevalence of 66%, with Pakistan reporting the highest (97%) and Japan the lowest (12%). These findings stress the importance of regular breaks, visual hygiene education, and ergonomic adjustments, particularly in developing countries where awareness remains low.
From a physiological standpoint, long-term visual health risks extend beyond temporary symptoms. Continuous exposure to blue light has been shown to disrupt circadian rhythms and sleep cycles Tosini (2016) and may contribute to early-onset macular degeneration and retinal stress Choi (2017). A study emphasized that the early initiation of screen use among adolescents and young adults could predispose them to irreversible visual changes over time Singh (2020).
Despite awareness of CVS in medical literature, actual preventive behaviour remains limited Mohan (2022) noted that only 18% of urban Indian users adhered to the 20-20-20 rule, and fewer than 10% used blue light filters or implemented ergonomic screen practices. This gap between knowledge and behaviour persists across educational and occupational sectors.
Global digital behaviour trends further reinforce the urgency of the issue. According to Statista (2023), global average daily screen time surpassed 7 hours in 2022, with Indian users reporting approximately 6.5 hours daily, especially among urban youth Duarte (2025). The World Health Organization has also cautioned against excessive sedentary screen time and recommends routine physical breaks, ergonomic setups, and screen usage guidelines WHO. (2020).
Thus, literature consistently demonstrates that CVS is a growing concern, particularly among younger populations who are chronically exposed to digital devices. Although existing studies have extensively documented the prevalence and symptoms of CVS, significant gaps remain in age-specific behavioural insights, ergonomic literacy, and preventive practices in the Indian context. This study aims to bridge these gaps by exploring the prevalence, contributing factors, and risk behaviours related to digital fatigue among 18–35-year-old screen users, providing a foundation for targeted interventions and awareness-building strategies tailored to modern digital lifestyles.
3. Aim and Specific Objectives
The study aims to assess the prevalence, symptoms, and contributing factors of Computer Vision Syndrome (CVS) and postural strain among screen users aged 18–35 years, and to evaluate their impact on visual health, physical discomfort, and overall well-being.
The specific objectives are: (i) To determine the prevalence and severity of Computer Vision Syndrome (CVS) among 18–35-year-old digital screen users; (ii) To identify common visual symptoms associated with prolonged screen exposure in this age group; (iii) To examine behavioural and ergonomic factors (e.g., screen time duration, posture, lighting, device type) that contribute to digital fatigue; (iv) To assess the awareness and adoption of preventive practices (e.g., screen breaks, ergonomic adjustments, eye exercises) among users.
4. Rationale
Today, digital devices have become integral to daily life, transforming the way individuals work, learn, and communicate. The 18–35 age group constitutes the most digitally engaged demographic, with many spending about 6–10 hours daily on screens for both professional and recreational purposes. While digital access brings undeniable benefits, this shift has also given rise to a modern health epidemic—digital fatigue, characterized by visual strain, musculoskeletal discomfort, and cognitive overload. Despite growing global recognition of Computer Vision Syndrome (CVS) and postural stress, there remains a significant lack of contextualized, India-specific research, especially targeting young adult populations in urban and semi-urban settings Roopa (2022). Most existing studies either focus narrowly on IT professionals or school children, or they fail to examine the combined impact of visual and postural strain, which are often interlinked in the real-world use of devices such as smartphones, tablets, and laptops. Furthermore, preventive awareness, ergonomic literacy, and protective behaviours—such as the 20-20-20 rule, correct seating posture, or screen time moderation—are strikingly low in India, even among educated users.
The long-term implications are alarming. Prolonged exposure to digital screens has been linked to retinal damage, circadian rhythm disruptions, early-onset myopia, and chronic neck and shoulder disorders. Left unaddressed, these issues will not only affect individual productivity and well-being but also place a substantial burden on public health systems and workplace efficiency. There is also a growing concern that the normalization of poor digital hygiene and sedentary screen-based routines could permanently alter health behaviours among youth.
This study is both timely and necessary. It fills a critical gap by exploring the prevalence, symptoms, behaviours, and ergonomic risk levels associated with digital fatigue in a high-risk, high-exposure age group. By combining survey data with postural observation using OWAS, it offers a multidimensional view of the issue—enabling the development of evidence-based interventions, awareness campaigns, and preventive strategies tailored to the Indian context.
This research is not merely exploratory—it is a call to action to recognize and address a rapidly growing, yet often overlooked, digital health concern of our time.
5. Research Methodology
An exploratory study was conducted among 160 computer users working in the fields of Finance, Digital Marketing, Software Industries, Gaming, and Influencing across three districts in Maharashtra. The participants, aged between 18 - 35 years, were randomly selected. Individuals with a minimum of 1 year (12 months) of relevant work experience, belonging to any ethnicity or BMI category, were included in the study. Participants who refused to sign the informed consent were excluded.
The tools used for data collection included a self-constructed questionnaire, OWAS (Ovako Working Posture Assessment System), observation, and personal interviews. The self-constructed questionnaire featured both open-ended and closed-ended questions. It consisted of four key parts. Part A covered the demographic profile of participants, which included details such as name, age, gender, qualification, income range, occupation, and work experience. It also captured their marital status, overall health rating, presence of any medical conditions, frequency of exercise, and type of employment. Part B focused on the work-related profile, highlighting aspects such as daily screen time, commonly used devices, work schedule, frequency of schedule changes, rest periods (both in number and duration), and frequency of breaks. It also explored the primary purpose of screen usage, blinking frequency, leisure screen time, nighttime screen use, and its impact on productivity or comfort. Part C addressed ergonomic and environmental factors, examining the participant’s workstation setup, screen distance, illumination levels, and screen positioning. It also considered ambient conditions, adherence to the 20-20-20 rule, and the OWAS (Ovako Working Posture Analysis System) score while using screens. Part D focused on symptoms experienced related to Computer Vision Syndrome (CVS), including eye strain, headaches, blurred vision, dry eyes, neck and shoulder pain, difficulty focusing, redness, light sensitivity, double vision, and watery eyes, with participants rating the severity of each symptom
The observation method was used to examine various work-related postures and workstation ergonomics, providing insights into the participants' work environment. To validate and refine the self-constructed questionnaire, a pilot study was conducted among 10 computer users from
The selected industries. The personal interview approach involved face-to-face interviews (20–25 minutes each), offering deeper insights into the prevalence of CVS symptoms, work stress, and ergonomic challenges. The collected data was coded into MS Excel 2019 and analyzed using simple statistical methods.
Despite the restrictions, the study successfully captured valuable data on CVS prevalence and its impact on computer users across multiple Sectors. It included not only office workers but also individuals from diverse sectors such as Information Technology (IT), finance, digital marketing, gaming, and social media influencing, all of whom rely heavily on digital tools.
6. Results AND Discussion
1) Demographic Profile of the Sample: The study sample comprised 160 screen users aged between 18 - 35 years, segmented into four distinct age groups. The largest proportion of participants belonged to the 31–35 years category (36%), closely followed by those aged 26–30 years (34%). Participants aged 21–25 years accounted for 22%, while the youngest group (18–20 years) formed the smallest segment at 8%. This distribution reflects a relatively balanced representation across early and mid-adulthood, ensuring a comprehensive view of digital fatigue among the working-age and student population.
In terms of self-rated health status, a majority of respondents across all groups categorized their health as either "Good" or "Very Good." Specifically:
· ‘Good’ health was reported most frequently by females aged 18–20 (24 participants) and males aged 31–35 (15 participants).
· ‘Very Good’ health was reported by a sizeable number of participants in each group, especially females aged 26–30 (15 participants) and 21–25 (12 participants).
· A very small number of participants (less than 3%) rated their health as ‘Fair’, ‘Poor’, or ‘Very Poor’, indicating that the overall sample was perceived to be in relatively good health at the time of the study.
Figure 1
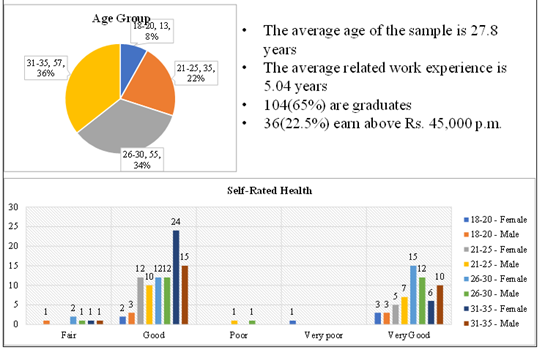
|
Figure 1 Profile of the Sample |
This demographic insight suggests that most participants did not have pre-existing health conditions, thereby making them an ideal cohort for assessing the impact of screen-induced visual and postural strain rather than attributing symptoms to underlying medical conditions. The inclusion of both genders across all age bands adds further depth and variability to the analysis, supporting age-and gender-specific insights into the prevalence and intensity of Computer Vision Syndrome and related ergonomic issues.
2) Work Profile: The occupational profile of the participants reveals several lifestyle and employment-related patterns that are highly relevant to the development of Computer Vision Syndrome (CVS). A majority of respondents (76%) were engaged in straight shift work, suggesting long, uninterrupted hours in front of screens. Only 18% worked rotational shifts, and 6% were in split shifts, which may offer marginal variations in screen exposure. Extended, continuous work shifts are a known risk factor for both visual strain and musculoskeletal fatigue, particularly in environments lacking ergonomic support or regulated break schedules.
The type of employment further reinforces this trend. An overwhelming 68% of participants were in permanent roles, with 18% in full-time temporary roles and only 3% in part-time positions. Permanent or full-time employment is often associated with greater screen-time obligations, especially in digital, desk-based, or remote work settings, increasing susceptibility to CVS over time.
Most notably, the data shows that 60% of respondents spend more than 8 hours per day on digital devices, while another 26% use screens for 6–8 hours daily. This means that 86% of the sample are exposed to digital screens for six hours or more per day—far exceeding the recommended screen time limits suggested by the World Health Organization (WHO) for visual health. This prolonged exposure heightens the risk of digital eye strain, blurred vision, dryness, headaches, and postural discomfort.
A critical compounding factor is the frequency of screen breaks. Despite high screen exposure, 40 participants (25%) reported that they ‘rarely’ take breaks, while another 16 (10%) never take breaks at all. Only 18% follow the recommended break intervals (every 20–30 minutes or every hour), which suggests a serious lack of preventive behaviour. Infrequent breaks impair tear production, reduce blink rate, and exacerbate both visual and physical fatigue.
Figure 2
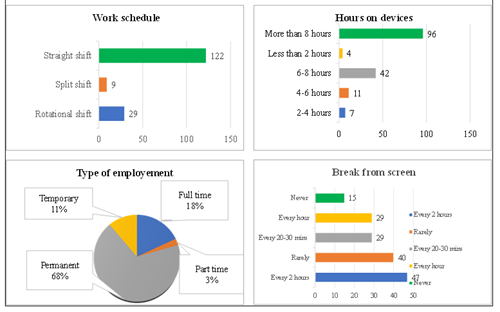
|
Figure 2 work Profile of the Sample |
Together, these findings highlight a high-risk work profile among participants, characterized by long working hours, full-time job roles, and excessive screen time with poor break habits. These conditions collectively create an occupational environment conducive to the early onset and chronic progression of CVS symptoms, particularly when not supported by workplace ergonomics or health education.
3) Reported
CVS Symptoms and Work-Related Correlates:
Analysis of the findings from Table 1 indicates a high prevalence of both visual and musculoskeletal symptoms consistent with Computer Vision Syndrome (CVS), underscoring the adverse effects of prolonged screen exposure in the 18–35-year-old working population.
· Severe Prevalence Symptoms (>65%): Neck pain (73.8%), headaches (70.6%), and eye strain (64.4%) emerged as the most frequently reported symptoms, placing them in the highest severity. category. These symptoms are closely linked to prolonged static posture, inadequate ergonomic setup, and non-compliance with screen break protocols, all evident in the study’s work-profile analysis. A large portion of the respondents (60%) reported working over 8 hours daily on screens, with 25% rarely taking breaks and 10% never taking breaks, amplifying the risk for cervical strain and visual overload.
· High-Moderate Prevalence Symptoms (60–64%): Although none of the symptoms fell within this range, eye strain at 64.4% borders this category and is typically the most direct manifestation of digital fatigue.
· Moderate Prevalence Symptoms (45–59%): Shoulder pain (51.3%), eye redness (37.5%), increased light sensitivity (35.6%), difficulty focusing (34.4%), and blurred vision (36.9%) fall within this band.
These outcomes reflect the dual strain on both ocular accommodation mechanisms and upper musculoskeletal structures, particularly for participants in straight-shift jobs (76%) and permanent employment roles (68%), where prolonged sitting and forward head posture are common.
The lack of ergonomic interventions, such as adjustable seating or eye-level monitors, could be contributing to these visual and postural disturbances.
· Mild to Moderate Symptoms (25–44%): Dry eyes (32.5%), double vision (29.4%), and watery eyes (43.8%) suggest tear film instability and ocular fatigue, frequently triggered by reduced blink rates and poor ambient lighting—common in indoor, screen-intensive work environments.
· Lower Prevalence (<25%): No symptoms were reported in this lowest category, indicating that all participants experienced at least moderate levels of CVS-related discomfort.
Table 1
|
Table 1 Reported Symptoms |
||
|
Symptoms |
f |
% |
|
Eye Strain |
103 |
64.4 |
|
Headache |
113 |
70.6 |
|
Blurred Vision |
59 |
63.9 |
|
Dry Eyes |
52 |
32.5 |
|
Neck Pain |
118 |
73.8 |
|
Shoulder Pain |
82 |
51.3 |
|
Dfficulty Focusing |
55 |
34.4 |
|
Eye Redness |
60 |
37.5 |
|
Increased light Sens |
57 |
35.6 |
|
Double Vision |
47 |
29.4 |
|
Watery eyes |
70 |
43.8 |
|
Code |
|
>65% |
|
60%-64% |
|
45%-59% |
|
25%-44% |
|
<24% |
The symptom distribution strongly correlates with participants’ long working hours, limited breaks, and dominant use of digital devices (especially among the 60% using screens for more than 8 hours daily). With permanent and full-time employees making up 86% of the sample, the occupational demands appear to significantly drive the onset, frequency, and intensity of CVS symptoms.
The musculoskeletal strain (neck and shoulder pain) is particularly elevated, aligning with findings from ergonomic literature that attribute static posture and repetitive stress without active intervention to upper-body discomfort.
4) Effects
of CVS Symptoms on Productivity and Screen-Time Practices:
· Screen Fatigue and Perceived Productivity Loss: 87(54%) acknowledged that screen usage has a negative impact on their daily productivity, while 46% did not report such an effect. This suggests that more than half of the participants experience a noticeable decline in task efficiency, focus, or energy, likely due to screen-induced fatigue, eye discomfort, or musculoskeletal strain.
· Symptom Worsening with Prolonged Screen Time: In the second chart, 84(52.5%) reported that their symptoms worsened after prolonged exposure to screens. This finding reinforces the association between extended screen durations and escalation of CVS symptoms, which can further reduce productivity, increase error rates, or necessitate more frequent rest breaks during work.
· Postural Discomfort and OWAS Scores: The OWAS (Ovako Working Posture Analysis System) scores, mapped against daily screen time, reveal a gradual deterioration in postural comfort as screen exposure increases. Notably:
42% of participants were in Score 2 (mild to moderate postural risk).
19% fell into higher-risk categories (Score 3 and 4), indicating significant postural strain, especially among those with more than 2 hours of screen time daily.
This reflects a strong correlation between poor posture, extended sitting, and reduced physical comfort, which collectively contribute to diminished productivity.
· Low Adoption of Preventive Practices (20-20-20 Rule): The 20-20-20 rule—an eye care strategy where users look away from the screen every 20 minutes at something 20 feet away for 20 seconds—was poorly followed.
Across all age groups:
Only 40 out of 160 participants (25%) reported using the 20-20-20 rule.
The highest compliance (15 users) was seen in the 31–35 age group, yet even here, nearly 74% did not follow the rule. The lack of adherence to preventive behaviours like this highlights a critical gap in digital hygiene awareness, increasing the likelihood of symptom exacerbation and productivity decline.
OWAS posture assessment was conducted and the results are presented below:
Table 2
|
Table 2 OWAS Score According to Screen Time |
|
|||||||||
|
Screen Time |
< 1 hour |
1-2 hours |
2-3 hours |
> 3 hours |
Total |
|||||
|
OWAS Score |
f |
% |
f |
% |
f |
% |
f |
% |
f |
% |
|
Score 1 |
12 |
7 |
27 |
17 |
20 |
13 |
3 |
2 |
62 |
39 |
|
Score 2 |
17 |
11 |
21 |
13 |
22 |
14 |
7 |
4 |
67 |
42 |
|
Score 3 |
6 |
4 |
4 |
3 |
8 |
5 |
5 |
3 |
23 |
14 |
|
Score 4 |
4 |
2 |
2 |
1 |
2 |
1 |
0 |
0 |
8 |
5 |
|
Total |
39 |
24 |
54 |
34 |
52 |
33 |
15 |
9 |
160 |
100 |
Table 3
|
Table 3 Interpretation Based on OWAS Risk Categories |
|||
|
OWAS Score |
Risk Category |
Meaning |
Required Action |
|
Score 1 |
Low Risk |
Natural posture; no
immediate threat to the musculoskeletal system |
No action required |
|
Score 2 |
Moderate Risk |
Potential for harm;
precautionary ergonomic measures advisable |
Corrective action in the near future |
|
Score 3 |
High Risk |
Harmful posture,
already affecting musculoskeletal health |
Corrective action as
soon as possible |
|
Score 4 |
Very High Risk |
Extremely harmful
posture and heavy physical load |
Immediate corrective
action is required |
Key Insights from OWAS Assessment:
1) Most
Participants Fall in Score 2 (Moderate Risk):
· 67 out of 160 participants (42%) were in Score 2, which signals a high need for preventive ergonomic measures.
· This is consistent across all screen time categories, showing posture risks are widespread even at lower screen durations.
2) Score
3 (High Risk) and Score 4 (Very High Risk):
· 23 participants (14%) had a Score 3, needing urgent posture corrections.
· 8 participants (5%) fell into Score 4, which demands immediate ergonomic intervention.
· High-risk postures are more common in those with 2–3 hours or more screen time.
3) Lower
Scores (1 and 2) Dominate Among Those Using Screens < 2 Hours:
· Those using screens for less than 1 hour/day had mostly Score 1 or 2 (29 out of 39), indicating relatively safer postures.
4) Prolonged
Screen Time Correlates with Higher OWAS Scores:
· Among participants using screens more than 3 hours/day, 53% (8 of 15) had Scores 3 or 4—a red flag for long-term health impacts.
7. Recommendations and Ergonomic Remedies for Preventing CVS and Work-Related Musculoskeletal Disorders
The findings from this study reveal a strong relationship between prolonged screen use, suboptimal workstation design, poor posture, and the prevalence of Computer Vision Syndrome (CVS) and musculoskeletal discomfort. A multi-pronged intervention strategy is recommended:
7.1. Workplace and Institutional Policy Interventions
· Mandatory Screen Hygiene Protocols: Enforce the 20-20-20 rule (every 20 minutes, look 20 feet away for 20 seconds).
· Structured Microbreaks: Introduce 5-minute posture and eye rest breaks every 30–60 minutes to prevent fatigue and strain.
· Digital Wellness Training: Conduct regular workshops on ergonomics, eye care, posture, and stress management.
· Task Rotation Models: Limit prolonged screen time through alternation of screen and non-screen tasks.
7.2. Ergonomic and Environmental Adjustments
·
Workstation Redesign:
Install height-adjustable chairs and desks.
Ensure optimal screen positioning (20–28 inches away at eye level).
Reorganize tools and equipment to reduce repetitive strain and awkward reach.
·
Visual Comfort Enhancements:
Use anti-glare screens and blue light filters.
Optimize lighting to minimize brightness contrast and glare.
·
Postural Comfort Aids:
Introduce sit-stand desks, footrests, and wrist supports.
Use anti-fatigue floor mats in standing workstations.
7.3. Risk-Specific Ergonomic Measures
·
For All Screen Users:
Provide training on neutral posture and movement strategies.
Promote awareness of ergonomics and musculoskeletal health.
·
For Moderate-Risk Group (OWAS Score 2):
Conduct regular workspace audits and posture assessments.
Recommend alternating between sitting and standing tasks.
·
For High-Risk Group (OWAS Scores 3 & 4):
Immediate ergonomic reconfiguration of workstations.
Enforce scheduled posture breaks and stretching exercises, especially targeting the neck, shoulders, and wrists.
Monitor for early symptoms of musculoskeletal disorders and intervene promptly.
7.4. Eye Health and Preventive Care
· Encourage annual eye exams, especially for users exceeding 6 hours of daily screen time.
· Promote frequent blinking, proper hydration, and the use of lubricating eye drops to combat dry eyes.
· Raise awareness of display settings, font sizes, and ambient light adjustments to reduce visual strain.
7.5. Technology-Enabled Solutions
· Deploy break reminder applications to prompt users to rest eyes and shift posture.
· Introduce wearables or smart screens that track posture, screen time, and notify users of unsafe digital behaviour.
7.6. User Education and Long-Term Behaviour Change
· Launch awareness campaigns highlighting the cumulative risks of CVS and poor ergonomics.
· Integrate digital well-being education into academic and workplace training programs.
· Encourage behaviour such as limiting late-night screen use, maintaining hydration, and incorporating movement into routine workflows.
By combining behavioural, design, environmental, and technological strategies, these recommendations aim to create healthier screen-based work environments and reduce the risk of both visual and postural disorders. This integrated approach is especially relevant for professionals in visually intensive and ergonomically challenging occupations.
· Informed Consent: Before their participation, all participants provided written informed consent, demonstrating their understanding of the study’s objectives, procedures, and potential risks.
CONFLICT OF INTERESTS
The authors disclose that they have no conflicting interests that could potentially influence the objectivity or integrity of the research conducted.
ACKNOWLEDGMENTS
The researchers express their sincere gratitude to the computer users who are corporate employees, gamers, and influencers for their valuable contributions to this research.
REFERENCES
Agarwal, S. e. (2021). Prevalence of Computer Vision Syndrome Among IT Professionals. Indian Journal of Occupational Health.
American Optometric Association. (2024). Computer vision syndrome.
Anbesu, E. W., a. L. (2023). Prevalence of Computer Vision Syndrome: A Systematic Review and Meta-Analysis. Pubmed Meta Analysis, 13(1). https://doi.org/10.1038/s41598-023-28750-6
Choi, Y. e. (2017). Effects of Blue Light on Retinal Health. Journal of Biomedical Optics, 22(12).
Computer Vision Syndrome - What is Computer Vision Syndrome? (2025).
Darshan, S. S. (2019). Prevalence of Computer Vision Syndrome Among Computer users of Kolar District. Innovastive Publication, 326-329. https://doi.org/10.18231/j.ijceo.2019.078
Duarte, F. (2025). Alarming Average Screen Time Statistics (2025).
Falguni, K. P. (2023). Assessment of Workplace Environment of BPO Employees. International Journal of Research and Analytical Reviews (IJRAR), 10(2), 6-10.
Kaur, K., G. B. (2022). Digital Eye Strain-A Comprehensive Review. Ophthalmol Ther, 1655-1680. https://doi.org/10.1007/s40123-022-00540-9
Lograj, M. e. (2014). Computer Vision Syndrome and Associated Factors Among Medical and Engineering Students. Annals of Medical and Health Sciences Research, 4(2), 179-185. https://doi.org/10.4103/2141-9248.129028
Mohan, A. e. (2022). Awareness of Digital Eye Strain Prevention Strategies Among Young Adults. Indian Journal of Public Health Research.
Portello, J. K., R. M. (2012). Computer-Related visual Symptoms in Office Workers. Ophthalmic Physiol Opt, 32(5), 375-382. https://doi.org/10.1111/j.1475-1313.2012.00925.x
Rao, R. (2020). Impact of Digital Technology on the
Postures Adopted by Teenagers. International Journal
of Future Generation Communication and Networking,
13(4), 34-46.
Roopa Rao, S. W. (2022). Perception of Discomfort Caused by Work Environment Factors Among Bank Clerks. International Journal of Multidisciplinary Educational Research (IJMER), 102-107.
Rosenfield, M. (2016). Computer vision syndrome: A Review of Ocular Causes and Potential Treatments. Ophthalmic and Physiological Optics, 36(5), 502-515. https://doi.org/10.1111/j.1475-1313.2011.00834.x
Sheppard, A. L. (2018). Digital Eye Strain: Prevalence, Measurement and Amelioration. BMJ Open Ophthalmology, 3(1). https://doi.org/10.1136/bmjophth-2018-000146
Shrestha, B. e. (2020). Musculoskeletal symptoms associated with mobile phone usage. International Journal of Occupational Safety and Ergonomics.
Silvani, M. I., W. R. (2022). The Influence of Blue Light on Sleep, Performance, and Wellbeing in Young Adults: A Systematic Review. Front Physiol, 13, 943108. https://doi.org/10.3389/fphys.2022.943108
Singh, R., & _. (2020). Visual Effects of Prolonged
Screen Exposure in Indian Youth. Journal of Clinical Ophthalmology and Research.
Tanaya Naik, R. R. (2022). Identifying
Ergonomics Risks Factors in
Bank Clerk Workstations.
International Journal for Innovative Research in Multidisciplinary Field (IJIRMF), 8(8), 104-110.
Tosini, G. e. (2016). Blue Light Hazards and Circadian Disruption. Progress in Retinal and Eye Research, 55, 92-107.
WHO. (2020). Guidelines on Physical Activity and Sedentary Behaviour.
 This work is licensed under a: Creative Commons Attribution 4.0 International License
This work is licensed under a: Creative Commons Attribution 4.0 International License
© Granthaalayah 2014-2025. All Rights Reserved.

