
RISK FACTOR ANALYSIS OF AUTISM IN CHILDREN AGED THREE TO TEN YEARS
Sarandha Sharma 1![]() , Dr. Ruby Sharma 2
, Dr. Ruby Sharma 2![]()
1 Research
Scholar, Teerhthankar Mahaveer University, Moradabad,
Uttar Pradesh, India
2 Assistant
Professor, Faculty of Education, Teerhthankar
Mahaveer University, Moradabad, Uttar Pradesh, India
|
|
|
ABSTRACT |
|
|
Autism Spectrum Disorder (ASD) is a complex neurodevelopmental condition that affects how individuals interact, communicate, and behave. The term “spectrum” emphasizes the wide variation in the type and severity of symptoms experienced. This study focuses on the emotional, social, and behavioral characteristics of children showing autistic traits. A group of 20 children was observed over one month during therapy sessions. An inventory based on the Modified Checklist for Autism in Toddlers (M-CHAT) was used to collect data. The study aimed to understand how emotional and behavioral challenges are linked to autism’s core features. The results showed that many children experienced emotional dysregulation—difficulty managing and expressing emotions appropriately. This often led to behavioral disturbances such as aggression, withdrawal, or tantrums. These behaviors were not random but closely tied to the child’s struggles with emotion regulation. Another important finding was the strong connection between problems in social communication and the presence of repetitive or stereotyped behaviors. For instance, children who found it hard to make eye contact or express themselves often repeated certain actions or phrases. This suggests that such behaviors might be ways for the child to cope with emotional discomfort or anxiety. The study highlights the need for therapeutic interventions that focus on improving emotional regulation and social communication skills. When children are better able to understand and manage their emotions, their disruptive behaviors may reduce. Likewise, helping them communicate more effectively can enhance their interactions with others. In conclusion, the research provides valuable insights into how emotional distress may manifest through behavioral symptoms in children with autism. These findings support the importance of early diagnosis and personalized therapies that address both emotional and social development, ultimately leading to better outcomes for children on the autism spectrum. |
|||
|
Received 15 February 2025 Accepted 21 March 2025 Published 16 April 2025 Corresponding Author Sarandha Sharma, sarandha.s@invertis.org DOI 10.29121/granthaalayah.v13.i3.2025.6029 Funding: This research
received no specific grant from any funding agency in the public, commercial,
or not-for-profit sectors. Copyright: © 2025 The
Author(s). This work is licensed under a Creative Commons
Attribution 4.0 International License. With the
license CC-BY, authors retain the copyright, allowing anyone to download,
reuse, re-print, modify, distribute, and/or copy their contribution. The work
must be properly attributed to its author.
|
|||
|
Keywords: Autism Spectrum Disorder, Emotional,
Social and Behavioral Disturbance |
|||
1. INTRODUCTION
Autism is a neurodevelopment disorder collectively called Autism Spectrum Disorder (ASD). In Greek auto means self and spectrum means a wide range of symptoms, skills, levels of impairment and disability. The key characteristics of autism are deficiency in social interaction, impaired communication skills and presence of restricted and repetitive interests or behavior. It is characterized by complex conditions that usually appear in early life before age three. Autistic children have significant impairment in social interaction. They make little eye contact, look and listen to people in their environment but they do not respond to others and respond less to their name. The autistic children show difficulties in imitating others or activities which are an integral part of learning about the things which lead to impairment in social interactions. In autistic children deficits in play skills cause inability to interact with same-age peers and be alone in leisure time. The deficits in play skills lead to problem in engaging in social imitation play which is needed for the development of social skills (Tarbox, Dixon, Stumey & Matson, 2014). Restricted, repetitive and stereotyped behaviour is one of the common symptoms seen in autistic child. The children show characteristics of rigidity by resisting to any changes in their environment. They have restricted interest in parts of objects rather than whole objects or function and are more attached to some inanimate objects. The autistic children engage in a repetitive and stereotypic motor mannerism which includes repeatedly flicking or flapping his or her fingers or rocking. Autistic children may also exhibit disturbed patterns of sensory perception. They are sometimes oversensitive to the stimuli that would not upset other children e.g. light touch or some clothes make pain to them. Sometimes they are under-sensitive to stimuli that would be painful to others. Autistic children also display problem behaviour including temper tantrums, aggression and self-injurious behaviour such as head banging or biting themselves.

· Emotion- Children with autism have a harder time with this development which includes having a difficult time understanding their own emotions. Depending on where they are on the spectrum some children might be able to express their feelings but are unable to describe what it is they are feeling.
· Social- Social development is about improving the well-being of every individual in society so they can reach their full potential. The success of society is linked to the well-being
· Social development means investing in people. It requires the removal of barriers so that all citizens can journey toward their dreams with confidence and dignity. It is about refusing to accept that people who live in poverty will always be poor. It is about helping people so they can move forward on their path to self-sufficiency.
· Behavior- In autism spectrum disorder (ASD), many individuals experience broader problem behavior at a level significant enough for families to seek further clinical assessment and intervention. The “problem behavior” as any significant emotional or behavioural issue captured by the Child Behavior Checklist (CBCL) including anxiety, depression, withdrawal, somatic complaints, problems with socialization, thought or attention, rule-breaking, and aggression. This study is aim to test the social, emotional and behavioural relationship of the children with autism.
The main focus in population is that all these participants were the children’s with special needs and we mainly concentrated on the children’s having the features of Autism. We excluded individuals who presented with other diagnoses such as multiple disabilities, motor disability, attention-deficit or hyperactivity disorder, obsessive–compulsive disorder, neurodegenerative diseases, and mental illnesses. We included only participants with ASD.
2. Objective of the study
The study aims to examine the social relationships,
emotional responsiveness, and behavior patterns of
children with autism, providing insights into their unique developmental
characteristics and interactions.
3. Methodology
A sample of 20 participants was recruited from
Rehabilitation Centre’s of Bareilly, Uttar Pradesh India. Both Male and Female
Children participated in this study. Under the study we used the purposive
sampling technique. The participants of the study belonged to differently sized
urban areas, and they represented both rural and urban areas. The children’s had previously been diagnosed by the mental
health services that are responsible for ascertaining the degree of disability
and dependency and consulted them therapies under the Rehabilitation
Centres.
Table 1
|
Table 1 Shows the Age Range and the Number of Participants
Both Boys and Girls. |
||
|
Sample:
Children with ASD |
||
|
N (%) |
20 (100%) |
20 (100%) |
|
Age, M (SD) |
5.7 (1.8844) |
|
|
Gender - Boys, N (%) |
9 (45%) |
|
|
Gender - Girls, N (%) |
11 (55%) |
|
|
Range |
Boy
child |
Girl
child |
|
3-4 |
0 |
5 |
|
4-5 |
2 |
2 |
|
5-6 |
2 |
1 |
|
6-7 |
1 |
0 |
|
7-8 |
3 |
2 |
|
8-9 |
1 |
0 |
|
9-10 |
0 |
1 |
|
ASD: autism spectrum disorder |
||
On the above Table 1 the age range of participants is presents along with the number of boys and girls. Under the table it is shown that in the study out of 20 participants from the age group of 3 to 10 years, 9 were boys and 11 were girls used as sample which were selected on the basis of random sampling method.
Figure 1

|
Figure 1 Shows Boys and Girls Participants’ Age Range |
For the present research a self made inventory with the help were made of M-Chat: The Modified Checklist for Autism in Toddlers, Revised with Follow-Up (M-CHAT-R/F; Robins, Fein, & Barton, 2009) to test the characteristics of Autism Spectrum Disorder (ASD) on the basis on only three dimensions – Behaviour, Emotional and Social. In the above is the graphical presentation of the table 1 in which age range and participants were shown. In the given graph color blue reflects boys participants and color orange reflects girls participants. This Inventory included total 30 questions in which first 10 questions were based on the Emotional dimension to test the emotional stability of the children. The next 10 questions were based on Social dimensions to test the social behavior of the children and last 10 questions were based on Behavioral dimensions of Autism to test the behavioural issues suffered by the children. As it is shown in above Table 1 that different age group children’s were participated in this study lies in between the age from 3 to 10 years only. The present study was conducted only after the consent of parents and authorities of rehabilitation centers for observation as well as to fill the inventory. The tests were administered in the educational centers by educational and behavioral science professionals who were knowledgeable about the behaviors of individuals with ASD (e.g., educational psychologists, therapists, and general psychologists). All the participating centers underwent an oral session that was organized by the researcher who described the purpose of the research study, the tests that were used, and instructions for test administration.
4. Analysis
Statistical analysis were analyzed by including covariance parameters between age and
each dimension of autism. We also analyzed whether
there were any gender differences using the same approach or not.
5. Results
We tested the risk factor of Autism in childhood under the
age group of 3 to 10 years with the help of self made
inventory with the help of M-Chat: The Modified Checklist for Autism in
Toddlers, Revised with Follow-Up (M-CHAT-R/F; Robins, Fein, & Barton, 2009)
mainly focused on the key dimensions of autism selected by the Researcher
itself i.e. Emotional, Social and Behavioural. The inventory is filled by the
parents on the basis of their general observations
over their child. The inventory included 30 Questions based on these above mentioned key dimensions and on the
basis of it marks have been given to each child and with their total score it
is tested that the child is having low, mild or severe features of autism with
the proper discussion with the therapists of rehabilitation centers.
The below mentioned tables shows the age group of the
participants, their responses to each dimensions,
their total score and the category he/she belongs too.
Table 2
|
Table 2 (Boys) Pre Test – Before Therapy of 1 Month |
||||||
|
Total participants=9 (Boys) |
Age group |
Emotional Variable |
Social Variable |
Behavior Variable |
Total score |
Level |
|
Participant
No. 1 |
3 -4
years |
Positive-
7 Negative – 3 |
Positive
- 9 Negative- 1 |
Positive
- 9 Negative- 1 |
25/30 |
High |
|
Participant
No. 2 |
3 -4
years |
Positive
- 2, Negative – 8 |
Positive
- 4, Negative – 6 |
Positive
- 3 Negative- 7 |
9/30. |
Low |
|
No participant |
4 - 5
years |
0 |
0 |
0 |
0 |
0 |
|
Participant
No. 3 |
5 - 6
years |
Positive
- 6 Negative- 4 |
Positive
- 5 Negative -5 |
Positive
- 5 Negative - 5 |
16/30 |
Mild |
|
Participant
No. 4 |
5 - 6
years |
Positive
- 9, Negative – 1 |
Positive
-9 Negative - 1 |
Positive
- 7 Negative- 3 |
25/30 |
High |
|
Participant
No. 5 |
6 -7
years |
Positive
- 4, Negative – 6 |
Positive
- 3 Negative- 7 |
Positive
- 7 Negative- 3 |
13/30 |
Mild |
|
Participant
No. 6 |
7 - 8
years |
Positive
- 7 Negative- 3 |
Positive
- 7 Negative- 3 |
Positive
- 7 Negative- 3 |
21/30 |
High |
|
Participant
No. 7 |
8 - 9
years |
Positive
- 7 Negative- 3 |
Positive
- 7 Negative- 3 |
Positive
-9 Negative - 1 |
23/30 |
High |
|
Participant
No. 8 |
8 - 9
years |
Positive
-4 Negative – 6 |
Positive
- 1 Negative - 9 |
Positive
- 3 Negative- 7 |
8/30. |
Low |
|
Participant
No. 9 |
8 - 9
years |
Positive
- 6 Negative – 4 |
Positive
- 8 Negative - 2 |
Positive
- 7 Negative- 3 |
21/30 |
High |
|
No participant |
9 - 10
years |
0 |
0 |
0 |
0 |
0 |
Table 3
|
Table 3 (Boys) Post-Test – After Therapy of 1 Month |
||||||
|
Total
participants=9 (Boys) |
Age
group |
Emotional
Variable |
Social
Variable |
Behavior Variable |
total
score |
Level |
|
Participant No. 1 |
3 -4 years |
Positive- 5 Negative – 3 |
Positive - 9 Negative- 1 |
Positive - 9 Negative- 1 |
23/30 |
High |
|
Participant No. 2 |
3 -4 years |
Positive - 2, Negative – 8 |
Positive - 4, Negative – 5 |
Positive - 3 Negative- 7 |
8/30. |
Low |
|
No participant |
4 - 5 years |
0 |
0 |
0 |
0 |
0 |
|
Participant No. 3 |
5 - 6 years |
Positive - 6 Negative- 4 |
Positive - 5 Negative -5 |
Positive - 5 Negative – 5 |
16/30 |
Mild |
|
Participant No. 4 |
5 - 6 years |
Positive - 9, Negative – 1 |
Positive -9 Negative – 1 |
Positive - 7 Negative- 4 |
26/30 |
High |
|
Participant No. 5 |
6 -7 years |
Positive - 4, Negative – 6 |
Positive - 3 Negative- 6 |
Positive - 7 Negative- 3 |
12/3 0 |
Mild |
|
Participant No. 6 |
7 - 8 years |
Positive - 7 Negative- 3 |
Positive - 7 Negative- 2 |
Positive - 7 Negative- 3 |
20/30 |
High |
|
Participant No. 7 |
8 - 9 years |
Positive - 7 Negative- 3 |
Positive - 4 Negative- 3 |
Positive -9 Negative – 1 |
20/30 |
Mild |
|
Participant No. 8 |
8 - 9 years |
Positive -4 Negative – 6 |
Positive - 1 Negative – 8 |
Positive - 3 Negative- 7 |
7/30. |
Low |
|
Participant No. 9 |
8 - 9 years |
Positive - 6 Negative – 4 |
Positive - 7 Negative – 2 |
Positive - 7 Negative- 3 |
20/30 |
High |
|
No participant |
9 - 10 years |
0 |
0 |
0 |
0 |
0 |
|
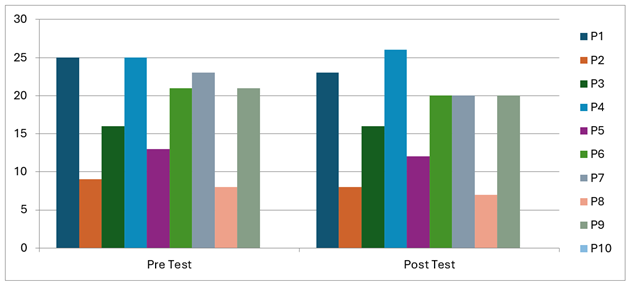
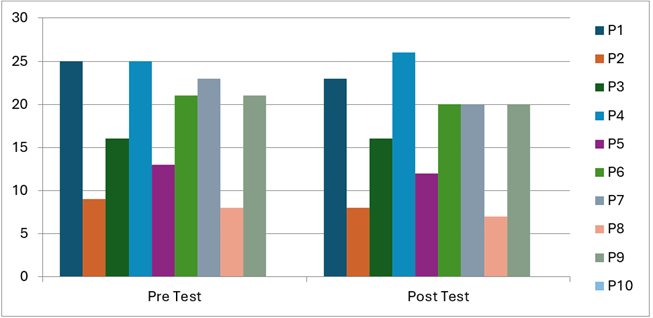
Here in chart positive
response as per the variable reflects to high or medium risk of autism and
negative response reflects to low risk of autism. Here in chart positive
response as per the variable reflects to high or medium risk of autism and
negative response reflects to low risk of autism. In chart the data is shown
before taking therapy session i.e. it is pre-test & hence it reflects
that participants 1 & 2 lies in the range of same age group of 3- 4 years
but have different level of autism whereas we didn’t find any male
participant under the age of 4 - 5 years, participants no. 3 & 4 lies in
the same age range of 5 – 6 years but have mild and high reflection of
autism, we found only 1 participant under the age of 6 – 7 & 7 -8 years
i.e. participant no. 5 & 6 which have mild & high risk of autism,
whereas participants no. 7, 8 & 9 are from the age group of 8 – 9 years
in which 2 participants shows same
risk of autism i.e. high and 1 participant shows low risk of autism and last
we didn’t find any male participant under the age group of 9 -10 years. So from the data we can understand that the level of risk
is variant as per their ages which can be low, mild and high, and now with
this data we can easily test the effect of therapy on different age groups in
post-test under the male category. |
||||||
Figure 2
|
Figure 2 Figure Shows Pre and Post-Test of Therapy Conducted for 1 Month on Male Participants |
Table 4
|
Table 4 (Girls) Pre -Test – Before Therapy of 1 Month |
||||||
|
Total participants=11 (Girls) |
Age Group |
Emotional Variable |
Social Variable |
Behavior Variable |
Total score |
Level |
|
Participant
No. 1 |
3 -4 years |
Positive
-7 Negative – 3 |
Positive
- 8 Negative - 2 |
Positive
- 8 Negative – 2 |
23/30 |
High |
|
Participant
No. 2 |
3 -4 years |
Positive
-8, Negative – 2 |
Positive
- 6, Negative - 4 |
Positive
- 7 Negative- 3 |
21/30 |
High |
|
Participant
No. 3 |
3 -4 years |
Positive
- 5 Negative- 5 |
Positive
- 3 Negative- 7 |
Positive
- 0 Negative - 10 |
8/30. |
Low |
|
Participant
No. 4 |
3 -4 years |
Positive
- 4 Negative – 6 |
Positive
- 5 Negative - 5 |
Positive
- 5 Negative – 5 |
14/30 |
Mild |
|
Participant
No. 5 |
3 -4 years |
Positive
- 4 Negative – 6 |
Positive
- 3 Negative- 7 |
Positive
- 5 Negative – 5 |
12/30. |
Mild |
|
Participant
No. 6 |
4 - 5 years |
Positive
- 3 Negative- 7 |
Positive
- 3 Negative- 7 |
Positive
- 6, Negative - 4 |
12/30. |
Mild |
|
Participant
No. 7 |
4 - 5 years |
Positive
- 6 Negative – 4 |
Positive
- 8 Negative - 2 |
Positive
- 5 Negative – 5 |
19/30 |
Mild |
|
Participant
No. 8 |
5 - 6 years |
Positive
-9 Negative – 1 |
Positive
- 4, Negative – 6 |
Positive
- 8 Negative – 2 |
21/30 |
High |
|
Participant
No. 9 |
6 -7 years |
Positive
-9 Negative – 1 |
Positive
- 7 Negative- 3 |
Positive
- 10 Negative- 0 |
26/30 |
High |
|
Participant
No. 10 |
7 - 8 years |
Positive
- 1 Negative- 9 |
Positive
- 4, Negative – 6 |
Positive
- 4, Negative - 6 |
9/30. |
Low |
|
No participant |
8 - 9 years |
0 |
0 |
0 |
0 |
0 |
Table 5
|
Table 5 (Girls) Post -Test – After Therapy of 1 Month |
|||||||
|
Total
participants=11 (Girls) |
Age
Group |
Emotional
Variable |
Social
Variable |
Behavior Variable |
total
score |
Level |
|
|
Participant No. 1 |
3 -4 years |
Positive -7 Negative – 3 |
Positive - 8 Negative - 2 |
Positive - 6 Negative - 2 |
21/30 |
High |
|
|
Participant No. 2 |
3 -4 years |
Positive -8 , Negative – 2 |
Positive - 6, Negative - 4 |
Positive - 6 Negative- 3 |
20/30 |
Mild |
|
|
Participant No. 3 |
3 -4 years |
Positive - 5 Negative- 5 |
Positive - 3 Negative- 7 |
Positive - 1 Negative -
10 |
9/30. |
Low |
|
|
Participant No. 4 |
3 -4 years |
Positive - 4 Negative – 6 |
Positive - 5 Negative - 5 |
Positive - 5 Negative - 5 |
14/30 |
Mild |
|
|
Participant No. 5 |
3 -4 years |
Positive - 4 Negative – 6 |
Positive - 3 Negative- 6 |
Positive - 5 Negative - 5 |
11/30. |
Mild |
|
|
Participant No. 6 |
4 - 5 years |
Positive - 3 Negative- 7 |
Positive - 3 Negative- 7 |
Positive - 4, Negative -
4 |
10/30. |
Mild |
|
|
Participant No. 7 |
4 - 5 years |
Positive - 6 Negative – 4 |
Positive - 8 Negative - 1 |
Positive - 5 Negative - 5 |
18/30 |
Mild |
|
|
Participant No. 8 |
5 - 6 years |
Positive -9 Negative – 1 |
Positive - 4, Negative - 6 |
Positive - 7 Negative - 2 |
20/30 |
Mild |
|
|
Participant No. 9 |
6 -7 years |
Positive -9 Negative – 1 |
Positive - 7 negative- 3 |
Positive - 8 Negative- 0 |
24/30 |
High |
|
|
Participant No. 10 |
7 - 8 years |
Positive - 1 Negative- 9 |
Positive - 4, Negative - 5 |
Positive - 4, Negative -
6 |
8/30. |
Low |
|
|
No participant |
8 - 9 years |
0 |
0 |
0 |
0 |
0 |
|
|
Participant No. 11 |
9 - 10 years |
Positive -9 Negative – 1 |
Positive -9 Negative - 1 |
Positive - 6 Negative - 2 |
24/30 |
High |
|
|
Here in chart positive
response as per the variable reflects too high or medium risk of autism and
negative response reflects to low risk of autism. Here in chart positive
response as per the variable reflects to high or medium risk of autism and
negative response reflects to low risk of autism. In chart the data is shown
before taking therapy session i.e. it is pre test
of female category only & hence it reflects that participants no. from 1
to 4 lies in the range of same age group of 3- 4 years but have different
level of autism i.e. low, mild & high, whereas participants no. 6 & 7
under the age of 4 - 5 years shows the same risk of autism, participants no.8
& 9 of 5 -6 & 6 -7 years age group have high risk. Participant 10
from the age group of 7 -8 years reflects low risk of autism whereas we
didn’t find any participant in the age of 8 -9 years and at last participant
no. 11 from 9 – 10 years shows the high risk of autism. So
from the data we can understand that the level of risk is variant as per
their ages which can be low, mild and high, and now with this data we can
easily test the effect of therapy on different age groups in post test under the female category. |
|||||||
Figure 3
|
Figure 3 Figure Shows Pre and Post-Test of Therapy Conducted for 1 Month on Girl’s Participants and its Graphical Presentation |
Table 6
|
Table 6 Score, Risk Categories and
Associative Actions. |
||||
|
Questions Category |
Response |
Score |
Category |
Actions |
|
Q. No. 1,4,17,20,21,22,23,25,26,28,29,
& 30 |
YES |
9 out of 30(10%-30%) i.e. Negative Score |
Low |
Reassured and given regular follow up |
|
10-20 out of 30 (30% - 70%) i.e. Positive Score |
Mild |
Referred to Neurodevelopment clinic |
||
|
Other Questions |
NO |
21and above out of 30 (70%-100%) i.e .Positive Score |
High |
Referred to autism multidisciplinary team
diagnostic clinic for further evaluation |
Children with a low risk score
were instructed by the therapists from their regular follow up. Children with a
medium risk score were referred to the Neuro developmental (ND) Clinic, run by
a consultant paediatrician who reviewed and verified responses using the
follow-up interview and tests. Children whose scores were in the high-risk
range were referred directly to AMTDC. The AMTDC consisted of a
multidisciplinary team including a consultant paediatrician, child
psychiatrist, clinical psychologist, speech therapist, occupational therapist,
and a social worker. Comprehensive diagnostic evaluations were in keeping with
recommendations for autism diagnosis, including - detailed health,
developmental and behavioural history, eliciting core diagnostic symptoms of
autism. In above Score, Risk Categories
and Associative Actions - M-CHAT Scoring and Referral Processes. For purposes
of our project with the guidelines of M-CHAT scores were classified as low risk
(i.e., negative score), medium risk, or high risk, as described in the M-CHAT
standard instructions.
6. Discussion and Conclusion
The aim of the study was to study the risk factor of autism in childhood under the age group of 3 to 10 years on both male child and female child based on three major dimensions of autism – Emotional, Social and Behavioral and the effect of therapy on the same dimensions after the period of one month. To analyze the effect of therapy on the autistic children we have observed them for one month and applied the same test again after taking parents in confidence which helps us to find out that in the period of one month is there any effect can be seen positively or negatively on child which may helpful for their further treatment. And it is also beneficial to notice that the same therapy could be continue or is there any changes required or not. From the above tables we are able to see that there is positive effect of therapy can be seen in just the period of one month for e.g. In male child participant no. 4 & 5 there is much changes can be notice like in participant no 4 there is negative changes means before the therapy session of one month he was on the score of 24 but it raised to 26 that makes his score more high which can be a serious matter to him and this only occur because he was not regularly taking his session (as asked by the parents) but on the other hand we can see that in participant no. 5 there is very positive changes noticed (last score was 23 and present score is recorded 20) i.e. from the stage of high he started to reducing his score and came in the category of mild and the reason is taking regular session of his therapy. The same type of changes we can see in female child table also in participants no. 2 & 8 they also resulted positively. Therefore the same score we can see in both the tables of male child as well as in female child that score is decreasing which is a good sign. And hence from the above discussion we can say that the effect of therapy going positive and if it’s going regular to the child than undoubtly the best result can be seen.
On the basis of the study conducted to test the risk factor of autism on the basis of three dimensions – Emotional, Social and Behavioral t it is found that a strong association was also identified between emotion regulation and social communication. Thus, individuals with ASD with more social communication skills show more emotional stability. Behaviour would act as an important signal for the detection of emotional distress or even a maladaptive mode of communication. Therefore, this fact has important repercussions for designing treatments that can mitigate self-injury behaviour and channel anxiety levels with other types of behaviours, such as stereotypes.
CONFLICT OF INTERESTS
None.
ACKNOWLEDGMENTS
None.
REFERENCES
Tyagi, A., & Jain, V. K. (2025). A Study of Professional Attitude of Teachers Trainees in Different Teacher Training Institutions. International Journal of Research -GRANTHAALAYAH, 13(3), 139-143. https://doi.org/10.29121/granthaalayah.v13.i3.2025.6026
Verma, M., & Sharma, R. (2021). A Brief Review on the Ancient Close Eastern Culture. ACADEMICIA: An International Multidisciplinary Research Journal, 11(11), 950-956. https://doi.org/10.5958/2249-7137.2021.02547.7
Verma, M., & Sharma, R. (2021). A Review on Women's Empowerment via Women's Network Learning. Asian Journal of Multidimensional Research, 10(12), 604-610. https://doi.org/10.5958/2278-4853.2021.01171.X
Verma, M., & Sharma, R. (2021). Education and Youth Crime: A Review of the Empirical Literature. Academicia: An International Multidisciplinary Research Journal, 11(12), 581-586.
 This work is licensed under a: Creative Commons Attribution 4.0 International License
This work is licensed under a: Creative Commons Attribution 4.0 International License
© Granthaalayah 2014-2025. All Rights Reserved.

