Homoeopathic management of targeted haemarthroses in inhibitor positive haemophiliac: A case report
Omkar Kumat 1![]()
![]() ,
Dr. Tapas Kundu 2
,
Dr. Tapas Kundu 2![]()
![]() , Gulfisha
Mirza 3
, Gulfisha
Mirza 3![]()
![]() , Rita Kundu 4
, Rita Kundu 4![]()
![]()
1 Communication
Consultant, Homoeopathy in Haemophilia, C/O Sakha the
Centre of Research and Charity, Upnagar, Nashik,
Maharashtra, India
2 Principal
Investigator, Homoeopathy in Haemophilia, C/O Sakha
the Centre of Research and Charity, Upnagar, Nashik,
Maharashtra, India
3 Research Associate, Homoeopathy in Haemophilia,
C/O Sakha the Centre of Research and Charity, Upnagar,
Nashik, Maharashtra, India
4 Coordinator, Homoeopathy in Haemophilia,
C/O Sakha the Centre of Research and Charity, Upnagar,
Nashik, Maharashtra, India
|
|
|
ABSTRACT |
|
|
Haemarthroses is common
presentation in haemophilia patient. Due to
recurrent use of clotting factor concentrates for treatment and prophylaxis,
of which about 20 % of patients produce antibodies to factor VIII and factor
IX. This results in development of inhibitors in such patients which complicates
the case even more. Homoeopathy the alternative form of treatment can be used
in such case. This case report presents the management of haemarthroses
in a haemophilia inhibitor. Well selected
homoeopathic similimum helped in reversing the haemophilic arthropathy in left knee joint of the patient
and even controlled the recurrence of the haemarthroses
in target joint. The result was assessed using Hemophilia joint health
assessment scale (HJHS). The result of before and after treatment was
extremely significant with a p value of 0.0009 The individual curative
response of the case was assessed using Modified naranjo
criteria for homoeopathic case reporting, casual attribution (MONARCH). |
|||
|
Received 29 November 2023 Accepted 30 December 2023 Published 13 January 2024 Corresponding Author Dr. Tapas
Kundu, dr_kundu2002@yahoo.co.in DOI 10.29121/granthaalayah.v11.i12.2023.5422 Funding: This research
received no specific grant from any funding agency in the public, commercial,
or not-for-profit sectors. Copyright: © 2023 The
Author(s). This work is licensed under a Creative Commons
Attribution 4.0 International License. With the
license CC-BY, authors retain the copyright, allowing anyone to download,
reuse, re-print, modify, distribute, and/or copy their contribution. The work
must be properly attributed to its author.
|
|||
|
Keywords: Homoeopathy, Hemophilia, Targetjoint, Inhibitor, Hemarthroses |
|||
1. INTRODUCTION
Bleeding episodes in muskulokeletal system is very common in haemophilia. About 80% occur within the joints mainly elbows, knees and ankles Rodríguez-Merchán (2019). When the haemorrhage persists or recurrent bleeds occur, intra-articular blood causes apoptosis of the chondrocytes. The synovial membrane usually hypertrophies as it reabsorbs blood, leading to accumalation of blood into joints. This a vicious cycle of chronic synovitis leads to joint destruction and classical haemophilic arthropathy, the involvement of target joint Valentino et al. (2012). Replacement of missing coagulation factors is usually the standard management in prevention and treatment of haemarthroses. Repeated exposure to replacement therapy leads to development of inhibitors against factor VIII (FVIII) or factor IX (FIX) in haemophilia patients. Haemarthroses is one of the most common complications in haemophilia and has major clinical and economic consequences Minno et al. (2010). About one-third of patients, following treatment with factor concentrates, usually develop an antibody (inhibitor) to that particular factor, making it inactive.This makes the patient more prone and at risk for life-threatening bleeding Wight & Paisley (2003).
2. Case Presentation
A pre-diagnosed case of severe haemophilia A and inhibitor positive presented on 24/01/2020 with left knee swelling on slightest trauma or strain.
Patient had vertigo since 2 days with restlessness due to pain. Aggravation-flexed knees, Amolieration-cold fomentation
Figure 1

|
Figure 1 Target joint - Lt. Knee |
Right knee joint=33cm
Left knee joint =39.5 cm
Past history Swelling of left knee joint intermittently since 2 years
Genetic and family history maternal
grandfather had haemophilia A
Local examination
Swelling with effusion
Leading to flexion and extension loss of left knee
Gait-limping
Walking, Stairs climbing, Running are not within normal limits according to global gait score (HJHS)
General examination-
Thirst-thirstless
All other general feature were within normal limits
Mind
Loquacious
Not serious about his studies
Miasmatic
analysis-Syco-syphillitic
3. Assessment with scales
Table 1
|
Table 1 Hemophilia Joint Health Score Before Treatment - Summary Score Sheet Morfini et al. (2007) |
||||
|
|
Left Knee |
Right Knee |
||
|
Swelling |
3 |
NE |
0 |
NE |
|
Duration (swelling) |
1 |
NE |
0 |
NE |
|
Muscle Atrophy |
0 |
NE |
0 |
NE |
|
Crepitus on motion |
1 |
NE |
0 |
NE |
|
Flexion Loss |
3 |
NE |
0 |
NE |
|
Extension Loss |
3 |
NE |
0 |
NE |
|
Joint Total |
15 |
|
0 |
|
Sum of Joint Totals -15
Global Gait Score - 4
|
HJHS Total Score =19 |
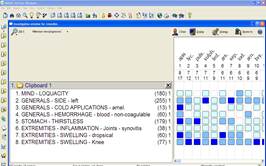
4. Rubrics and Remedial analysis
Figure 2
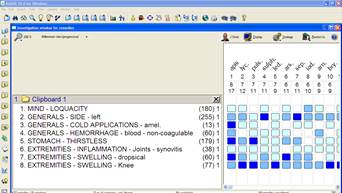
|
Figure 2 Repertorial Totality |
Rx,
1) Apis Mel 30,5 doses 24 hourly in sacchrum lactis.
2) Placebo in 30 number globules, 2 drachm bottle to be taken 4 pills BD.
Table 2
|
Table 2 Follow Up Chart |
|||
|
Date |
Symptoms |
Justification and Image |
Medicine |
|
03/04/2021 |
The patient was lost to follow up for
almost an year due COVID-19 restrictions. When he returned his left knee swelling
was almost the same. Right knee joint=34cm Left knee joint =39.5 cm |
Figure 3 Repertorial Sheet |
Apis Mellifica
30 in saclac powder 3 doses 24 hourly Placebo in 30 number globules,2 drachm
bottle to be taken 4 pills BD |
|
14/06/2021 |
Partial relief Right knee joint=34cm Left knee joint =37cm |
Figure 4 Repertorial Sheet |
Phytolacca Decandra
30 in saclac powder 3 doses 24 hourly Placebo in 30 number globules,2 drachm
bottle to be taken 4 pills BD |
|
18/07/2021 |
Right knee joint=34.5 cm Left knee joint =38 cm |
Figure 5 Repertorial Sheet |
Strontium Carbonicum
30 in saclac powder 3 doses 24 hourly Placebo in 30 number globules,2 drachm
bottle to be taken 4 pills BD |
|
03/9/2021 |
Swelling of left knee increased since
2days. Earlier the swelling had reduced to and
flexion increased. Right knee joint-35.5 Left Knee joint-37.5cm |
Figure 6 Repertorial Sheet |
Clemitis Erecta 30 in saclac powder 3 doses 24 hourly Placebo in 30 number globules,2 drachm
bottle to be taken 4 pills BD |
|
20/11/2021 |
Right knee joint=36.5 Left knee joint =36.5 |
Figure
7 Left Knee Measurement
Figure 8 Right Knee Measurement
Figure 9 Both the Knees (Normal) |
Sulphur 0/1 ,3 doses 24 hourly. Placebo in 30 number globules,2 drachm
bottle to be taken 4 pills BD |
|
11/04/2022 |
Target joint completely resolved. No recurrence of bleeding since last 6
months. |
Figure 10 Follow Up After 6 Months |
Placebo in 30 number globules,2 drachm
bottle to be taken 4 pills BD |
Table 3
|
Table 3 Hemophilia Joint Health Score After Treatment - Summary Score Sheet-14 |
||||
|
|
Left Knee |
Right Knee |
||
|
Swelling |
0 |
NE |
0 |
NE |
|
Duration (swelling) |
0 |
NE |
0 |
NE |
|
Muscle Atrophy |
0 |
NE |
0 |
NE |
|
Crepitus on motion |
0 |
NE |
0 |
NE |
|
Flexion Loss |
0 |
NE |
0 |
NE |
|
Extension Loss |
0 |
NE |
0 |
NE |
|
Joint Pain |
0 |
NE |
0 |
NE |
|
Strength |
0 |
NE |
0 |
NE |
|
Joint Total |
0 |
|
0 |
|
Sum of Joint Totals -0
+ = Global Gait Score 0
|
HJHS Total Score =0 |
5. Discussion
Haemarthroses, that is intra-articular haemorrhages are a frequent finding usually observed in patients with haemophilia Rodriguez-Merchan et al. (2011), Buzzard & Beeton (2008), Buzzard & Jones (1988). The extravasation of blood into the joint is the most important event that leads to development of haemophilic arthropathy Hermans et al. (2011), Lafeber et al. (2008), Roosendaal et al. (2008). The functional prognosis becomes very poor once arthropathy develops Nilsson et al. (1992). Long-term prophylaxis aimed in order to establish factor levels over 1 IU dL, if started at an early age, prevents the onset of chronic haemophilic arthropathy Roosendaal et al. (2008). However, after the replacement therapy about 10% and 30% of patients with severe haemophilia A and 2–5% of patients with severe haemophilia B usually develop anti FVIII and anti FIX antibodies respectively Rodriguez-Merchan et al. (2003) When present, these inhibitors inactivate the biological activity of infused FVIII or FIX, making the patient refractory to treatment Morfini et al. (2007), Lamba et al. (2020). Haemophilic arthropathy along with inhibitors is quite a challenge.
This case presents homoeopathic management of case of
chronic haemarthroses in haemophilia inhibitor. Left
knee joint over the period of two years was found to be the target joint. Rest
all joints were normal functionally and anatomically. This target joint
swelling had completely hampered the routine of the patient. As the left leg
had flexion and extension loss to severe degree even daily chores seemed
difficult. Walking, climbing stairs, running was obscured. When the patient
presented at Homoeopathy in haemophilia research centre, he was already
diagnosed with inhibitor. The case was thoroughly analysed. Left knee joint was
severely swollen (Figure 1) with effusion. After
a thorough case taking Apis mellifica 30 was
prescribed. Later on, due to COVID-19 pandemic the patient was lost to follow
up. Over the time recurrent haemorrhages had caused chronic haemophilic
arthropathy in
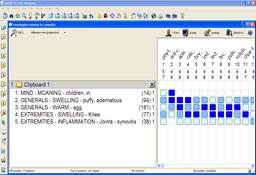
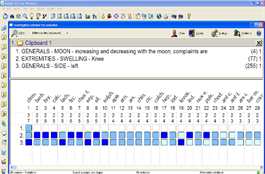
over left knee. Apis mellifica, strontium carb and phytolacca were prescribed (Table 2) with moderate changes in the patient. Each medicine though brought down the swelling to moderate degree, but recurrence of swelling at target joint was the concern and hence it was changed time to time. Fresh anamnesis was done and typical symptom of aggravation during full moon and new moon was noticed. New totality was formed (Figure 6) and Clematis Erecta was prescribed. This brought about the desired results and the swelling was completely resolved. Both the knees measured equal and were normal functionally and anatomically. After the pathology had resolved, sulphur 0/1 which was found to be constitutional was prescribed to inhibit the recurrence of swelling. For next 6 months regular follow, up was taken. No episodes of recurrence of bleeding at target joint were seen.
The syco-syphillitic changes
that had occured in target joint were completely
reversed. The joint health was evaluated using Hemophilia
joint health assassment score (HJHS). The difference
of before and after treatment using HJHS score was tested with paired t-test. The two-tailed P value equals 0.0009
By conventional criteria, this difference is considered to be extremely
statistically significant. Modified Naranjo criteria for homoeopathy,
casual attribution (MONARCH) St-Louis et al. (2022)
inventory was used to assess curative response of the case. The score of
MONARCH is 10. Reporting of the case strictly adheres to HOM-CASE-CARE Van Haselen
(2016)
guidelines.
6. Conclusion
Haemarthroses was effectively managed in a diagnosed inhibitor positive Haemophiliac with homoeopathic Intervention.
7. Declaration of Patient Consent
The authors
testify that they have obtained proper patient and parents’ consent in written
format from the patient. The patient has given consent for clinical information
and images for the sake of scientific interest and publication of data.
8. Patients perspective
The case being a paediatric case, mothers perspective was taken. According to her slightest trauma frequently caused swelling in left knee joint. Homoeopathic treatment reduced frequency and reversed the hemophilic arthropathy. It has brought his sons routine back to normal.
CONFLICT OF INTERESTS
None.
ACKNOWLEDGMENTS
None.
REFERENCES
Buzzard, B. M., & Jones, P. M. (1988). Physiotherapy Management of Haemophilia: An Update. Physiotherapy, 74(5), 221-226. https://doi.org/10.1016/S0031-9406(10)63535-3
Buzzard, B., & Beeton, K. (2008). Physiotherapy Management of Haemophilia. John Wiley & Sons.
Hermans, C., De Moerloose, P., Fischer, K., Holstein, K., Klamroth, R., Lambert, T., Lavigne-Lissalde, G., Perez, R., Richards, M., Dolan, G. & European Haemophilia Therapy Standardisation Board. (2011). Management of Acute Haemarthrosis in Haemophilia a Without Inhibitors: Literature Review, European Survey and Recommendations. Haemophilia, 17(3), 383-392. https://doi.org/10.1111/j.1365-2516.2010.02449.x
Lafeber, F. P. J. G., Miossec, P., & Valentino, L. A. (2008). Physiopathology of Haemophilic Arthropathy. Haemophilia, 14, 3-9. https://doi.org/10.1111/j.1365-2516.2008.01732.x
Lamba, C. D., Gupta, V. K., van Haselen, R., Rutten, L., Mahajan, N., Molla, A. M., & Singhal, R. (2020). Evaluation of the Modified Naranjo Criteria for Assessing Causal Attribution of Clinical Outcome to Homeopathic Intervention as Presented in Case Reports. Homeopathy, 109(04), 191-197. https://doi.org/10.1055/s-0040-1701251
Minno, M. D., Minno, G. D., Capua, M. D., Cerbone, A. M., & Coppola, A. (2010). Cost of Care of Haemophilia with Inhibitors. Haemophilia, 16(1), e190-e201. https://doi.org/10.1111/j.1365-2516.2009.02100.x
Morfini, M., Haya, S., Tagariello, G., Pollmann, H., Quintana, M., Siegmund, B., Stieltjes, N., & Tusell, J. (2007). European study on orthopaedic status of haemophilia patients with inhibitors. Haemophilia, 13(5), 606-612. https://doi.org/10.1111/j.1365-2516.2007.01518.x
Nilsson, I. M., Berntorp, E., Löfqvist, T., & Pettersson, H. (1992). Twenty-five Years' Experience of Prophylactic Treatment in Severe Haemophilia A and B. Journal of Internal Medicine, 232(1), 25-32. https://doi.org/10.1111/j.1365-2796.1992.tb00546.x
Rodriguez-Merchan, E. C., Wiedel, J. D., Wallny, T., Hvid, I., Berntorp, E., Rivard, G. E., Goddard, J., Querol, F., & Caviglia, H. (2003). Elective Orthopaedic Surgery for Inhibitor Patients. Haemophilia, 9(5), 625-631. https://doi.org/10.1046/j.1365-2516.2003.00803.x
Rodriguez-Merchan, E., Jimenez-Yuste, V., Aznar, J. A., Hedner, U., Knobe, K., Lee, C. A., Ljung, R., Querol, F., Santagostino, E., Valentino, L. A. & Caffarini, A. (2011). Joint protection in haemophilia. Haemophilia, 17, 1-23. https://doi.org/10.1111/j.1365-2516.2011.02615.x
Rodríguez-Merchán, E. C. (2019). The Role of Orthopaedic Surgery in Haemophilia: Current Rationale, Indications and Results. EFORT Open Reviews, 4(5), 165-173. https://doi.org/10.1302/2058-5241.4.180090
Roosendaal, G., Jansen, N. W. D., Schutgens, R., & Lafeber, F. P. J. G. (2008). Haemophilic Arthropathy: the Importance of the Earliest Haemarthroses and Consequences for Treatment. Haemophilia, 14, 4-10. https://doi.org/10.1111/j.1365-2516.2008.01882.x
St-Louis, J., Abad, A., Funk, S., Tilak, M., Classey, S., Zourikian, N., McLaughlin, P., Lobet, S., Hernandez, G., Akins, S., Wells, A. J., Manco-Johnson, M., John, J., Austin, S., Chowdary, P., Hermans, C., Nugent, D., Bakeer, N., Mangles, S., Hilliard, P., Blanchette, V.S., Feldman, B. M., & Feldman, B. M. (2022). The hemophilia joint health score version 2.1 validation in adult patients study: a multicenter international study. Research and practice in thrombosis and haemostasis, 6(2). https://doi.org/10.1002/rth2.12690
Valentino, L. A., Hakobyan, N., Enockson, C., Simpson, M. L., Kakodkar, N. C., Cong, L., & Song, X. (2012). Exploring the Biological Basis of Haemophilic Joint Disease: Experimental Studies. Haemophilia, 18(3), 310-318. https://doi.org/10.1111/j.1365-2516.2011.02669.x
Van Haselen, R. A. (2016). Homeopathic Clinical Case Reports: Development of a Supplement (HOM-CASE) to the CARE Clinical Case Reporting Guideline. Complementary Therapies in Medicine, 25, 78-85. https://doi.org/10.1016/j.ctim.2015.12.019
Wight, J., & Paisley, S. (2003). The Epidemiology of Inhibitors in Haemophilia A: A Systematic Review. Haemophilia, 9(4), 418-435. https://doi.org/10.1046/j.1365-2516.2003.00780.x
 This work is licensed under a: Creative Commons Attribution 4.0 International License
This work is licensed under a: Creative Commons Attribution 4.0 International License
© Granthaalayah 2014-2024. All Rights Reserved.